The Definition of Low Birth Weight Can Be Found in the Notes for Subheading
Birth Weight
From Embryology
Jump to:navigation, search
| Embryology - fifteen February 2022 |
|---|
| Google Interpret - select your linguistic communication from the list shown below (this volition open a new external folio) |
| العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not exist accurate. (More than? Nigh Translations) |
Educational Use Only - Embryology is an educational resource for learning concepts in embryological evolution, no clinical information is provided and content should not be used for any other purpose.
Introduction

There are a variety of prenatal techniques for estimating approximate birth weight that are relevant for preterm, term and prolonged pregnancy. Ultrasound two- and three-dimensional scanning methods are the basis of almost current techniques. There are likewise standard autopsy weight curves that have been developed from second and third trimester fetal and too neonatal autopsy. Low birth weight is accurately defined as a statistical indicator for development. High birthweight definition on the other hand varies in the literature and between countries with a lower cut-off in a higher place 4000 gm or 4500 gm.
At birth, infants are generally weighed as shortly as possible and may too exist monitored during the neonatal period. In Australia, the average birthweight for all babies born: (1991) three,350 grams, (2004 three,370 grams and (2015)[1] 3,327 grams. Also in 2022 6.5% (19,852) of liveborn babies were of low birthweight.[1]
- Links: ultrasound | DOHAD | maternal diabetes | macrosomia
| Birth Links: nascency | Lecture - Nascency | caesarean | preterm birth | nativity weight | macrosomia | Nativity Statistics | Australian Nascency Data | Developmental Origins of Health and Disease (DOHAD) | Neonatal Diagnosis | Apgar test | Guthrie examination | neonatal | stillbirth and perinatal death | ICD-10 Perinatal Menstruation | Category:Nascence | ||
|
Some Recent Findings
- New Australian Birthweight Centiles [2] "All singleton births in Commonwealth of australia of 23-42 completed weeks' gestation and with spontaneous onset of labour, 2004-2013. Births initiated past obstetric intervention were excluded to minimise the influence of decisions to deliver modest for gestational age babies before term. Current birthweight centile charts probably underestimate the incidence of intra-uterine growth restriction because obstetric interventions for delivering pre-term small for gestational age babies depress the curves at earlier gestational ages. Our curves circumvent this trouble past excluding intervention-initiated births; they also incorporate more contempo population data. These updated centile curves could facilitate more than authentic diagnosis of small for gestational historic period babies in Commonwealth of australia."
- Fetal brain development in small-for-gestational historic period (SGA) fetuses and normal controls [three] "Objective To appraise whether fetal encephalon structures routinely measured during the second and tertiary trimester ultrasound scans, particularly the width of the cavum septi pellucidi (CSP), differ between fetuses minor for gestational historic period (SGA), fetuses very pocket-size for gestational historic period (VSGA) and normal controls. Methods In this retrospective study, nosotros examined standard ultrasound measurements of 116 VSGA, 131 SGA fetuses and 136 normal controls including the caput circumference (HC), transversal diameter of the cerebellum (TCD), the sizes of the lateral ventricle (LV) and the cisterna magna (CM) from the second and 3rd trimester ultrasound scans extracted from a clinical database. We measured the CSP in these archived ultrasound scans. The HC/CSP, HC/LV, HC/CM and HC/TCD ratios were calculated as relative values independent of the fetal size. Results The HC/CSP ratio differed notably betwixt the controls and each of the other groups (VSGA P = 0.018 and SGA P = 0.017). No notable difference in the HC/CSP ratio between the VSGA and SGA groups could be found (P = 0.960). The HC/LV, HC/CM and HC/TCD ratios were like in all the three groups. Conclusion Relative to HC, the CSP is larger in VSGA and SGA fetuses than in normal controls. Even so, there is no notable difference betwixt VSGA and SGA fetuses, which might be an indicator for abnormal encephalon evolution in this group."
- Diagnosing Small for Gestational Historic period during 2d trimester routine screening: Early sonographic cluesFatihoglu East & Aydin Due south. (2020). Diagnosing Small for Gestational Age during second trimester routine screening: Early sonographic clues. Taiwan J Obstet Gynecol , 59, 287-292. PMID: 32127152 DOI. "Small for gestational historic period (SGA) is mostly defined as nascency weight being at or beneath the tenth percentile. Children with SGA have a higher gamble for complications. In that location is a need for early on predictors, as the accurate diagnosis rate is only 50%. In the current study, we aimed to evaluate diagnostic performance of ultrasound (US)/color Doppler ultrasound (CDUS) parameters (umbilical vein-UV, correct portal vein-RPV diameter/menses charge per unit, and portal sinus-PS bore) examined at 20-22 gestational calendar week as SGA diagnostic factors. CONCLUSION: UV, RPV, and PS diameters tin be before predictors for SGA diagnosis. Routinely evaluation of these parameters during second trimester screening can increment SGA diagnosis rates and serve for early diagnose."
- Impact of biometric measurement fault on identification of modest- and big-for-gestational-age fetuses [4] OBJECTIVES: First, to obtain measurement-error models for biometric measurements of fetal abdominal circumference (AC), head circumference (HC) and femur length (FL), and, 2nd, to examine the touch of biometric measurement mistake on sonographic estimated fetal weight (EFW) and its effect on the prediction of small- (SGA) and large- (LGA) for-gestational-age fetuses with EFW < 10th and > 90th percentile, respectively. CONCLUSIONS: Measurement fault in fetal biometry causes substantial fault in EFW, resulting in misclassification of SGA and LGA fetuses. The extent to which improvement can be accomplished through effective quality balls remains to be seen merely, every bit a first stride, information technology is important for practitioners to understand how biometric measurement error impacts the prediction of SGA and LGA fetuses."
| More contempo papers |
|---|
| This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
More? References | Discussion Folio | Periodical Searches | 2022 References | 2022 References Search term: Birth Weight | Small-scale for Gestational Historic period | Big for Gestational Age | Low Birth Weight | Very Low Nativity Weight | Extremely Low Nascency Weight | High Birth Weight Birth Weight Z-score | |

| Older papers |
|---|
| These papers originally appeared in the Some Recent Findings table, but equally that list grew in length have now been shuffled down to this collapsible table. Run across besides the Give-and-take Folio for other references listed by yr and References on this electric current page.
|
Birth Weight Classifications
The primary causes of VLBW are premature birth (born <37 weeks gestation, and oft <xxx weeks) and intrauterine growth restriction (IUGR), usually due to problems with placenta, maternal health, or to nativity defects. Many VLBW babies with IUGR are preterm and thus are both physically small and physiologically immature.
| | no colour | ||||||||||
| Birth weight (grams) | less 500 | 500 – 999 | 1,000 – 1,499 | ane,500 – 1,999 | 2,000 – 2,499 | 2,500 – 2,999 | 3,000 – 3,499 | 3,500 – 3,999 | 4,000 – 4,499 | 4,500 – 4,999 | 5,000 or more |
| Classification | | | | | | ||||||
Extremely Depression Nativity Weight
- Less than 500 grams (1 lb i oz or less)
- 500 – 999 grams (1 lb 2 oz – 2 lb 3 oz)
Very Low Nascency Weight
- i,000 – i,499 grams (two lb 4 oz – 3 lb 4 oz)
Depression Birth Weight
- 1,500–1,999 grams (3 lb v oz – 4 lb 6 oz)
- 2,000–2,499 grams (4 lb 7 oz – 5 lb eight oz)
Normal Birth Weight
- ii,500–2,999 grams (5 lb nine oz – 6 lb 9 oz)
- 3,000–iii,499 grams (half-dozen lb x oz – 7 lb 11 oz)
- 3,500–three,999 grams (7 lb 12 oz – eight lb xiii oz)
High Nascency Weight
- 4,000–4,499 grams (eight lb xiv oz – ix lb 14 oz)
- 4,500–4,999 grams (ix lb 15 oz – 11 lb 0 oz)
- 5,000 grams or more (11 lb one oz or more)
- see also macrosomia
Weight Conversions
| Extremely Low Birth Weight | Very Depression Nativity Weight | Low Birth Weight | Normal Birth Weight | High Birth Weight (macrosomia) |
|---|---|---|---|---|
|
|
|
|
|
No Background Version
| Nativity weight (grams) | less 500 | 500 – 999 | ane,000 – 1,499 | 1,500 – ane,999 | 2,000 – 2,499 | 2,500 – 2,999 | 3,000 – iii,499 | 3,500 – 3,999 | iv,000 – iv,499 | 4,500 – four,999 | five,000 or more |
| Classification | | | | | | ||||||
Small for Gestational Age
Pocket-sized for gestational age (SGA) is a term used for infants as having a birth weight more than ii standard deviations (SD) below the hateful or less than the 10th percentile for the gestational age (GA). WHO birthweight definitions are low birthweight as less than ii,500 grams, very low birthweight is less than 1,500 grams and extremely low birthweight: less than 1,000 grams. Growth brake can be symmetrical (dull development with limited brain growth) or asymmetrical (head circumference and length are preserved and brain growth is relatively spared).
- Symmetric SGA (Weight, head circumference and length all below the tenth percentile) tin be due to chromosomal abnormalities, intrauterine infection, severe placental insufficiency and or a constitutionally small babe.
- Asymmetric SGA (Weight below the 10th percentile) can be due to interference with placental function and or interference with maternal health in 3rd trimester.
There are a large number of known relationships betwixt low birth weight and both maternal and fatal abnormalities, a few examples are shown below.
Z-score
The nativity weight Z-score is a predictor of agin neonatal outcome in astringent placental insufficiencies.[fourteen] For an individual nascency weight, a z-score of -1 is one standard difference beneath the mean birth weight of the accomplice.
The Z-score nomenclature organisation can be used to compare a kid or a group of children to the reference population.
The Z-score (SD-score) = (observed value - median value of the reference population) / standard difference value of reference population.
- Z-score scale is linear - therefore a fixed interval of Z-scores has a fixed peak departure in cm, or weight difference in kg, for all children of the same age.
- Z-scores are sex-contained - allows evaluation of children's growth status past combining sex and age groups.
- Z-scores allow statistical calculations - such every bit means, standard deviations, and standard error to classify a population'south growth status.
The Z-score classification system can also be used for population-based assessments, for case to monitor nutritional status malnutrition, wellness and within nutrition centers.
The z-score differences (Zdiff) uses standard deviation scores to analyze changes in growth for a particular observation menstruation.
- Links:WHO
Fetal Gastroschisis
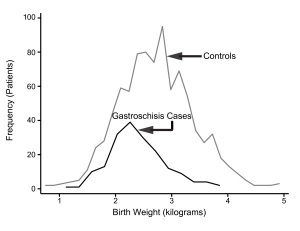
Gastroschisis Birth Weight Graph
Gastroschisis patients are commonly small-scale for gestational age (SGA, birth weight < 10th centile). Frequency line graphs of the nascence weight distribution.[15]
The abnormality is usually situated to the right of the umbilicus and abdominal contents, mainly gastrointestinal, are found outside the anterior torso wall. Tin occur in isolation and also in association with other gastrointestinal anomalies (intestinal atresia, perforation, necrosis or volvulus). Defects in other organ systems accept been reported in up to 35% of children.
Maternal Elevated Testosterone
Maternal elevated testosterone levels is associated with depression birth weight in humans. Hyperandrogenism associated with polycystic ovarian syndrome (PCOS) and pre-eclampsia have a higher prevalence of small-for-gestational age newborns. A rat model written report suggests that maternal testosterone does not cross the placenta, to directly suppress fetal growth, but affects nutrient delivery to the fetus by downward-regulating specific amino acid transporter activeness.[16]
High Altitude
Altitude affects growth patterns measured in a a contempo Peruvian study of 63,620 healthy infants built-in at low (150 grand) and loftier (3000-4400 thou) distance were compared.[17] They found that in the third trimester "Hateful and median nativity weight differences between those built-in at low and high altitudes reached statistical significance after 35 and 33 weeks, respectively."
Canada
Definition: Alive births with a nascence weight of 4,500 grams or more, expressed equally a percentage of all live births with known birth weight.
High nascency weight can result in complications for the infant and female parent during birth and may exist associated with an increased hazard of diabetes.
- Links: Canada Statistics | Statistics Canada, Vital Statistics, Birth Database.
Australia - Indigenous
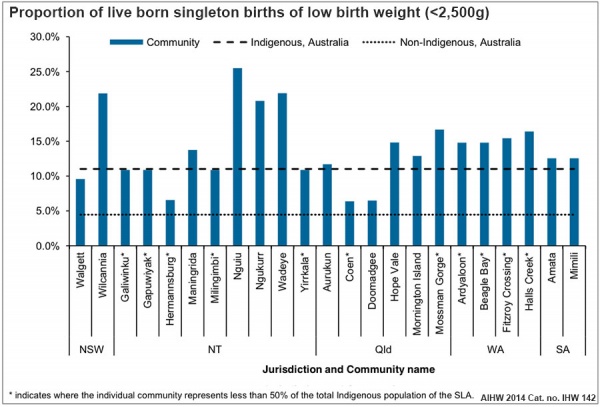
Australian low birth weight (2008–2009)[18]
Information in graphs below from AIHW 2022 Report, Birthweight of babies born to Indigenous mothers.[ten]
- Links: Australian Statistics | Preterm Birth | SmokingBirth weight reference percentiles for Chinese===
Mainland china
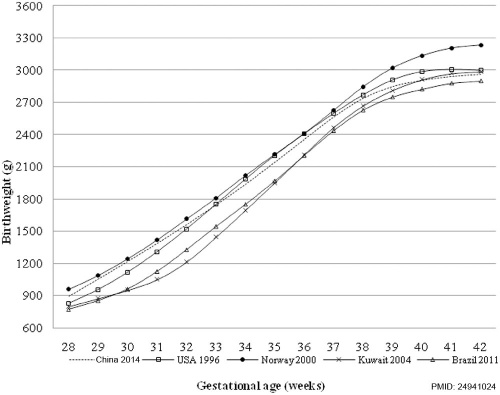
Nascence weight reference percentiles for Chinese[12] "There have been moderate increases in birth weight percentiles for Chinese infants of both sexes and most gestational ages since 1980s, suggesting the importance of utilizing an updated national reference for both clinical and enquiry purposes."
- Links: China Statistics
References
- ↑ i.0 1.1 Australian Institute of Health and Welfare 2017. Commonwealth of australia'southward mothers and babies 2015—in brief. Perinatal statistics series no. 33. Cat no. PER 91. Canberra: AIHW.
- ↑ Joseph FA, Hyett JA, Schluter PJ, McLennan A, Gordon A, Chambers GM, Hilder L, Choi SK & de Vries B. (2020). New Australian birthweight centiles. Med. J. Aust. , , . PMID: 32608051 DOI.
- ↑ Jacob E, Braun J, Oelmeier K, Köster HA, Möllers M, Falkenberg M, Klockenbusch W, Schmitz R & Hammer K. (2020). Fetal brain development in small-for-gestational age (SGA) fetuses and normal controls. J Perinat Med , , . PMID: 32126016 DOI.
- ↑ Wright D, Wright A, Smith Eastward & Nicolaides KH. (2020). Touch on of biometric measurement error on identification of pocket-size- and large-for-gestational-age fetuses. Ultrasound Obstet Gynecol , 55, 170-176. PMID: 31682299 DOI.
- ↑ Freedman AA, Hogue CJ, Marsit CJ, Rajakumar A, Smith AK, Goldenberg RL, Dudley DJ, Saade GR, Silver RM, Gibbins KJ, Stoll BJ, Bukowski R & Drews-Botsch C. (2019). Associations Betwixt the Features of Gross Placental Morphology and Birthweight. Pediatr. Dev. Pathol. , 22, 194-204. PMID: 30012074 DOI.
- ↑ Takemoto R, Anami A & Koga H. (2018). Human relationship between birth weight to placental weight ratio and major congenital anomalies in Japan. PLoS Ane , thirteen, e0206002. PMID: 30346975 DOI.
- ↑ Salcedo-Bellido I, Martínez-Galiano JM, Olmedo-Requena R, Mozas-Moreno J, Bueno-Cavanillas A, Jimenez-Moleon JJ & Delgado-Rodríguez M. (2017). Association between Vitamin Intake during Pregnancy and Risk of Small for Gestational Age. Nutrients , 9, . PMID: 29168736 DOI.
- ↑ Paltiel O, Tikellis Thou, Linet Thou, Golding J, Lemeshow S, Phillips G, Lamb K, Stoltenberg C, Håberg SE, Strøm M, Granstrøm C, Northstone K, Klebanoff Yard, Ponsonby AL, Milne E, Pedersen M, Kogevinas M, Ha Due east & Dwyer T. (2015). Birthweight and Childhood Cancer: Preliminary Findings from the International Childhood Cancer Cohort Consortium (I4C). Paediatr Perinat Epidemiol , 29, 335-45. PMID: 25989709 DOI.
- ↑ Upadhyay Yard, Pourcyrous M, Dhanireddy R & Talati AJ. (2015). Outcomes of neonates with birth weight⩽500 1000: a twenty-year experience. J Perinatol , 35, 768-72. PMID: 25950920 DOI.
- ↑ 10.0 10.one AIHW 2014. Birthweight of babies built-in to Indigenous mothers. Cat. no. IHW 138. Canberra: AIHW. Viewed five Baronial 2022 http://world wide web.aihw.gov.au/publication-particular/?id=60129548202
- ↑ Li Z, Wang YA, Ledger W & Sullivan EA. (2014). Birthweight percentiles by gestational age for births following assisted reproductive engineering in Australia and New Zealand, 2002-2010. Hum. Reprod. , 29, 1787-800. PMID: 24908671 DOI.
- ↑ 12.0 12.1 Ye J, Zhang Fifty, Chen Y, Fang F, Luo Z & Zhang J. (2014). Searching for the definition of macrosomia through an result-based approach. PLoS Ane , 9, e100192. PMID: 24941024 DOI.
- ↑ Adams-Chapman I, Hansen NI, Shankaran S, Bell EF, Boghossian NS, Murray JC, Laptook AR, Walsh MC, Carlo WA, Sánchez PJ, Van Meurs KP, Das A, Unhurt EC, Newman NS, Ball MB, Higgins RD & Stoll BJ. (2013). X-twelvemonth review of major birth defects in VLBW infants. Pediatrics , 132, 49-61. PMID: 23733791 DOI.
- ↑ da Silva FC, de Sá RA, de Carvalho PR & Lopes LM. (2007). Doppler and birth weight Z score: predictors for adverse neonatal consequence in severe fetal compromise. Cardiovasc Ultrasound , 5, fifteen. PMID: 17374167 DOI.
- ↑ Payne NR, Simonton SC, Olsen S, Arnesen MA & Pfleghaar KM. (2011). Growth restriction in gastroschisis: quantification of its severity and exploration of a placental cause. BMC Pediatr , 11, 90. PMID: 22004141 DOI.
- ↑ Sathishkumar Grand, Elkins R, Chinnathambi V, Gao H, Hankins GD & Yallampalli C. (2011). Prenatal testosterone-induced fetal growth restriction is associated with down-regulation of rat placental amino acrid send. Reprod. Biol. Endocrinol. , 9, 110. PMID: 21812961 DOI.
- ↑ Gonzales GF & Tapia Five. (2009). Birth weight charts for gestational age in 63,620 healthy infants born in Peruvian public hospitals at low and at high distance. Acta Paediatr. , 98, 454-viii. PMID: 19038011 DOI.
- ↑ AIHW 2014. Health indicators for Remote Service Delivery communities: a summary written report. Cat. no. IHW 142. Canberra: AIHW. Viewed five November 2022 http://www.aihw.gov.au/publication-detail/?id=60129548650.
Reviews
Manufactures
Hemming K, Hutton JL & Bonellie S. (2009). A comparing of customized and population-based birth-weight standards: the influence of gestational age. Eur. J. Obstet. Gynecol. Reprod. Biol. , 146, 41-v. PMID: 19581044 DOI.
Search Pubmed
Search Pubmed: Low Birth Weight | small-scale for gestational age
External Links
External Links Observe - The dynamic nature of the internet may mean that some of these listed links may no longer function. If the link no longer works search the spider web with the link text or name. Links to any external commercial sites are provided for data purposes simply and should never exist considered an endorsement. UNSW Embryology is provided as an educational resource with no clinical information or commercial affiliation.
- METoER (Commonwealth of australia) Nativity—nascence weight, lawmaking N
- CDC (USA) Pediatric Diet Surveillance System - Birthweight
- WHO Low Birthweight (2004) PDF
| Nascency Terms | ||
|---|---|---|
| ||
|
Glossary Links
- Glossary: A | B | C | D | E | F | Thousand | H | I | J | Thousand | Fifty | M | N | O | P | Q | R | S | T | U | Five | Westward | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2022, February xv) Embryology Nativity Weight. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Birth_Weight
-
- What Links Hither?
- © Dr Mark Hill 2022, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G
Source: https://embryology.med.unsw.edu.au/embryology/index.php/Birth_Weight
0 Response to "The Definition of Low Birth Weight Can Be Found in the Notes for Subheading"
Post a Comment